
New Scientist
Wed, 07 Aug 2019 00:01 UTC
Have we found the true cause of diabetes, stroke and Alzheimer’s?
Does this one microbe cause heart disease, stroke, Alzheimer’s, diabetes, Parkinson’s, pre-term birth, pancreatic cancer, and kidney disease… and does that mean we can beat them?
For decades, health experts have been lecturing us about our bad habits, blaming them for the surge in “lifestyle diseases”. These often come on as we age and include heart disease, Alzheimer’s, type 2 diabetes and some cancers. Worldwide, 70 per cent of all deaths are now attributed to these conditions. In the U.K., it is a whopping 90 per cent.
Too much red meat, too little fruit and veg, smoking, drinking, obesity and not enough exercise appear to make all these diseases more likely – and having any of them makes getting the others more likely. But no one really knows why, and we still haven’t worked out what causes any of them. Alzheimer’s is now one of the U.K.’s biggest killers, yet the main hypothesis for how it originates imploded this year after drugs based on it repeatedly failed. High blood cholesterol is blamed for heart attacks, except most people who have heart attacks don’t have it.
What we do know is that these conditions usually start causing symptoms later in life, and their prevalence is skyrocketing as we live longer. They all turn inflammation, the method our immune system uses to kill invaders, against us. And, by definition, these diseases aren’t communicable. They are down to bad habits and unlucky genes, not germs. Right?
Not necessarily. In disease after disease, we are finding that bacteria are covertly involved, invading organs, co-opting our immune systems to boost their own survival and slowly making bits of us break down. The implication is that we may eventually be able to defeat heart attacks or Alzheimer’s just by stopping these microbes.
Until now, bacteria’s involvement completely eluded us. That’s because they tend to work very slowly, stay dormant for long periods or hide inside cells. That makes them difficult to grow in culture, once the gold standard for linking bacteria to disease. But now D.N.A. sequencing has revealed bacteria in places they were never supposed to be, manipulating inflammation in just the ways observed in these diseases.
The findings are so contrary to received wisdom and emerging in so many diseases, each with its own separate research community, that awareness of all this is only starting to hit the mainstream (See “Germ theory”). And predictably, as with any paradigm shift, there is resistance.
But some researchers, frustrated by years of failure to find causes, and therefore real treatments, for the diseases of ageing, are cautiously excited. And with reason: this could change everything.
The worst culprits, which seem to play a role in the widest range of ailments, are the bacteria that cause gum disease. This is the most widespread disease of ageing – in fact, “the most prevalent disease of mankind”, says Maurizio Tonettiat the University of Hong Kong. In the U.S., 42 per cent of those aged 30 or above have gum disease, but that rises to 60 percent in those 65 and older. It has been measured at 88 percent in Germany.
Strikingly, many of the afflictions of ageing – from rheumatoid arthritis to Parkinson’s – aremore likely, more severe, or both, in people with gum disease. It is possible that some third thing goes wrong, leading to both gum disease and the other maladies. But there is increasing evidence that the relationship is direct: the bacteria behind gum disease help cause the others.
Circumstantial evidence is certainly damning. In the U.S., states that put federal Medicaid funds towards people’s dental costs, including those related to preventing or treating gum disease, ultimately pay between 31 and 67 per cent less than states that don’t, to help those people later with heart attacks, diabetes, strokes and cancer. Private insurance companies report similar patterns, says David Ojcius at the University of the Pacific in San Francisco.
But how can the bacteria that cause gum disease play a role in all these conditions? To answer that, we have to look at how they turn the immune system against us.
Your mouth hosts more than 1000 species of bacteria, in a stable community where potential bad actors are kept in check by peaceful bacteria around them. Elsewhere in the body, including on the skin or the lining of the gut, communities of bacteria live on a continuous sheet of cells, where the outermost layer is constantly shed, getting rid of invasive bacteria. But your teeth can’t cast off a layer like that, says Tonetti. There, the bacteria live on a hard surface, which pierces through the protective outer sheet of cells.
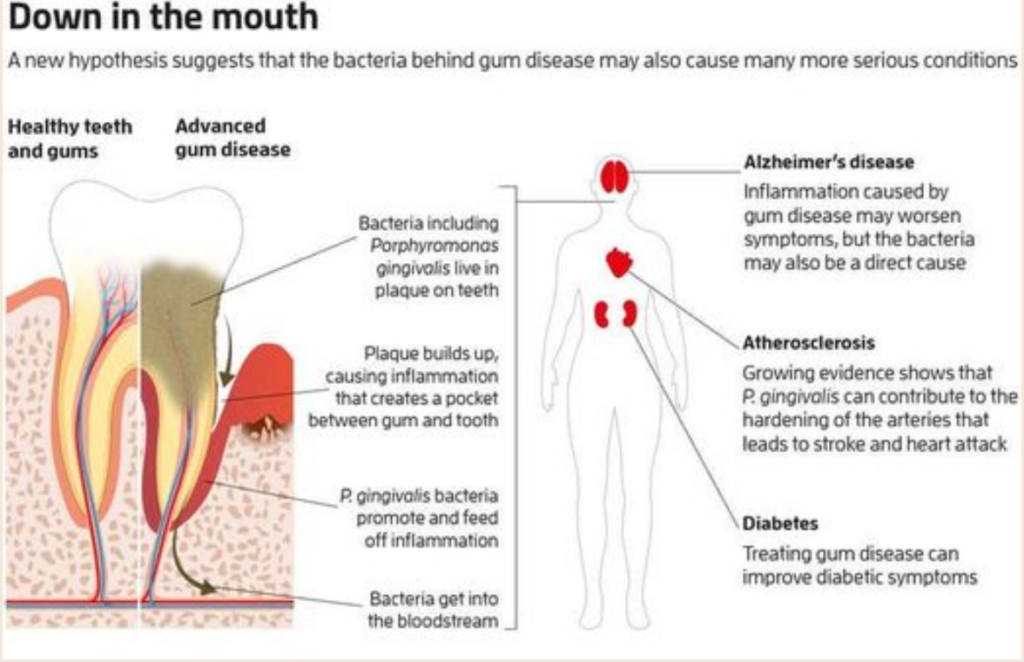
When the plaque the bacteria on your teeth live in builds up enough to harden and spread under the gum, it triggers inflammation: immune cells flood in and destroy both microbes and our own infected cells (see Diagram). If this goes on too long, an oxygen-poor pocket develops between gum and tooth. A handful of bacteria take advantage of this and multiply. One of them, Porphyromonas gingivalis, is especially insidious, disrupting the stable bacterial community and prolonging inflammation.
This might seem a strange thing to do. Most pathogens try to block or avoid inflammation, which normally kills them before it shuts down again. Starting in our 30s and 40s, this shutdown begins failing, leading to the chronic inflammation involved in diseases of ageing. No one knows why.
P. gingivalismay have a hand in it. It actually perpetuates inflammation by producing molecules that block some inflammatory processes, but not all of them, says Caroline Genco of Tufts University in Massachusetts. The resulting weakened inflammation never quite destroys the bacteria, but keeps trying, killing your own cells in the process. The debris is a feast for P. gingivalis, which, unlike most bacteria, needs to eat protein.
The destruction also liberates the iron that bacteria need and which the body therefore normally keeps locked up. “These bacteria manipulate their interaction with the host immune response to enhance their own survival,” says George Hajishengallis at the University of Pennsylvania.
Gum control
Eventually, the infected tooth falls out – but long before that P. gingivalis escapes into the bloodstream. There your immune system makes antibodies against it, which usually defend us from germs. But P. gingivalis antibodies seem to be more a mark of its passing than protection. People with these antibodies are actually more likely to die in the next decade than those with none, and more likely to get rheumatoid arthritis or have a heart attack or stroke.
This could be because, once in the blood, P. gingivalischanges its surface proteins so it can hide inside white blood cells of the immune system, says Genco. It also enters cells lining arteries. It remains dormant in these locations, occasionally waking to invade a new cell, but otherwise remaining hidden from antibiotics and immune defences. However, even hunkered down within our cells, P. gingivalis continues to activate or block different immune signals, even changing a blood cell’s gene expression to make it migrate to other sites of inflammation, where the bacteria can hop out and feast again.
One explanation for why gum disease makes you more likely to get conditions like diabetes and Alzheimer’s disease is that it adds to your general “inflammatory load”. But P. gingivalis may act more directly too: the bacteria have been detected in inflamed tissue in the brain, aorta, heart, liver, spleen, kidneys, joints and pancreas in mice and, in many cases, humans.
Master of concealment
If the bacterium Porphyromonas gingivalis is partly to blame for a wide range of inflammatory diseases such as Alzheimer’s and heart disease, why not just kill it? Unfortunately, it is brilliant at dodging our defences: lurking inside cells where antibodies can’t reach it, and often lying dormant, making it invisible to antibiotics, which mostly attack bacteria as they divide.
We could vaccinate against P. gingivalis, but vaccines work by inducing antibodies. People with gum disease already make antibodies against the bacteria, but these seem to do little to stop it.
It may be better to have the antibodies early and stop P. gingivalis invading our mouths when we are young. Eric Reynolds at the University of Melbourne is running a clinical trial of a vaccine that targets gingipains, the protein-digesting enzymes that P. gingivalis makes. Caroline Genco of Tufts University in Massachusetts is also working on an anti-gingipain vaccine. “The key is to prevent it ever colonising,” she says.
The trouble is, many of us already host the bacteria. Routine gum abrasion, through eating or brushing your teeth, can release the microbes into your bloodstream, even if you don’t have gum disease. There it can spread throughout the body and promote inflammation.
In studies by the company Cortexyme, antibiotics killed P. gingivalis in mice, but it rapidly became resistant. To limit resistance, instead of trying to kill the bacteria, it may be better to block its ability to cause disease. Cortexyme has a drug that does this by blocking gingipains. In mice, it reversed Alzheimer’s-like brain damage without driving resistance in P. gingivalis, and in a small trial in humans it improved inflammation and some measures of cognition. A large trial is now under way.
But as all these diseases involve inflammation, why not just block that? If we did, it could leave you open to the germs that this immune response does fight off or block other vital things that immune signals do. That’s why some companies are working on drugs to block only specific inflammatory signals. But tampering with our complex immune systems without doing damage – as P. gingivalis shows – will be a significant challenge.The strongest case against P. gingivalis is as a cause of Alzheimer’s disease. This constitutes more than two-thirds of all dementia, now the fifth largest cause of death worldwide. It was long blamed on the build-up of two brain proteins, amyloid and tau. But that hypothesis is crumbling: people with dementia may lack this build-up, while people with lots of the proteins may have no dementia – and most damningly, no treatments reducing either have improved symptoms.
In fact, the build-up of beta amyloid plaques in the brain, rather than causing dementia, may be a natural defense mechanism against microbes. See: How an outsider in Alzheimer’s research bucked the prevailing theory (and he’s probably right)
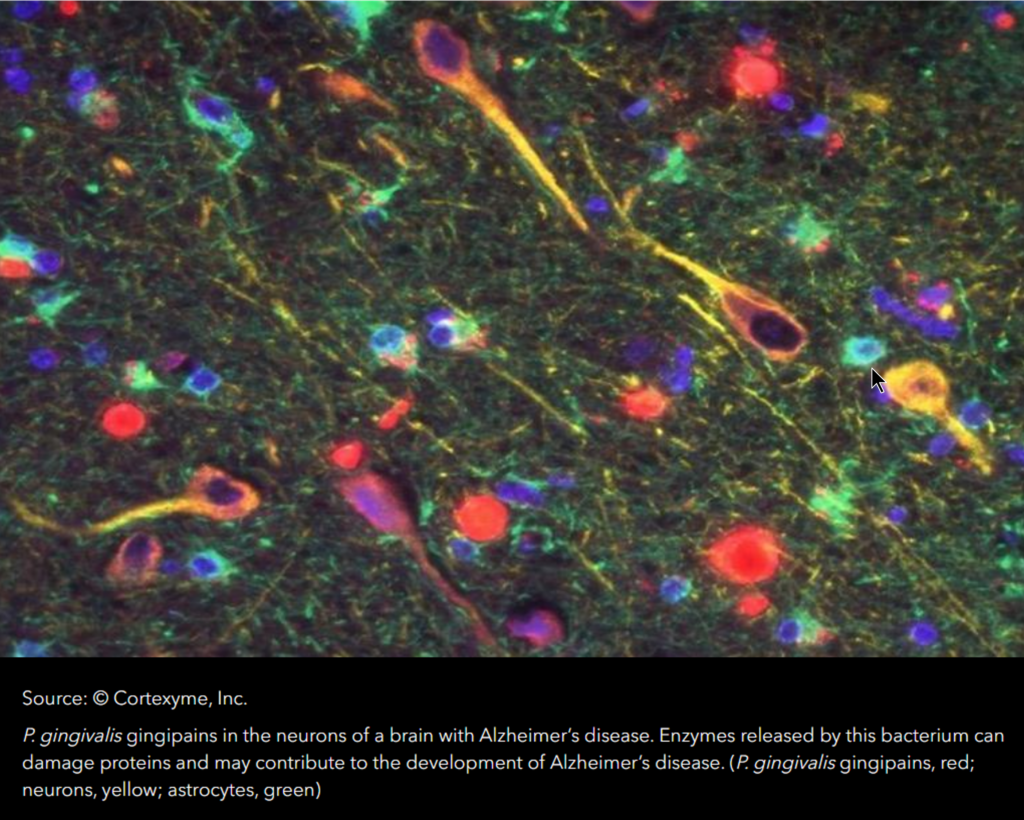
Then, in January, teams at eight universities and the San Francisco company Cortexyme found a protein-digesting enzyme called gingipain, produced only by P. gingivalis, in 99 per cent of brain samples from people who died with Alzheimer’s, at levels corresponding to the severity of the condition. They also found the bacteria in spinal fluid. Giving mice the bacteria caused symptoms of Alzheimer’s, and blocking gingipains reversed the damage.
Moreover, half of the brain samples from people without Alzheimer’s also had gingipain and amyloid, but at lower levels. That is as you would expect if P. gingivalis causes Alzheimer’s, because damage can accumulate for 20 years before symptoms start. People who develop symptoms may be those who accumulate enough gingipain damage during their lifetimes, says Casey Lynch at Cortexyme.
Still, dementia researchers have questioned how a bacterial cause can account for genetic risk factors for Alzheimer’s. But it may actually explain them, according to a team in Sweden. The people with the highest genetic risk produce a particular form of an immune protein called ApoE that is destroyed in the disease. Last year, Swedish researchers discovered that gingipains are better at destroying that particular ApoE than other forms.
P. gingivalis may literally break our hearts too. There is growing evidence for a causal link to atherosclerosis, or “hardening of the arteries”. Researchers have found P. gingivalis in the fatty deposits that line arterial walls and cause blood clots. When bits of clots clog blood vessels in hearts or brains, they cause heart attack and stroke.
The bacteria trigger the molecular changes in artery linings that are typical of atherosclerosis, says Genco. We have also found that P. gingivalis creates the lipoproteins thought to trigger atherosclerosis, causes it in pigs and affects arteries much like high fat diets. Lakshmyya Kesavalu at the University of Florida, who has cultured viable P. gingivalis from the atherosclerotic aortas of mice, calls the bacteria “causal“.
The American Heart Association agrees that gum disease is an “independent” risk factor for cardiovascular disease, but doesn’t call it causal. It argues that although treating gum disease improves hardened arteries, no studies have found that it reduces heart attacks or strokes. But, according to Steve Dominy at Cortexyme, that could be because, while gum treatment helps arteries by easing inflammatory load, it doesn’t eradicate the P. gingivalis already in the blood vessels. Clinical trials are needed to firm up the connection, but these are expensive and difficult – especially when the bacterial hypothesis is still in its early days.
The link is clearer for type 2 diabetes, in which people lose sensitivity to insulin and eventually can’t make enough to control blood sugar. It is currently a pandemic, blamed on the usual lifestyle suspects.
Diabetes worsens gum disease, because high blood sugar levels hurt immune cells. But gum disease also worsens diabetes, and treating it helps as much as adding a second drug to the regimen taken by someone with the condition, according to the American Academy of Periodontology. Treatment is now recommended by diabetes associations, yet none of them list gum disease as a risk factor. As with other conditions, there is evidence that P. gingivalis isn’t promoting diabetes just by adding to the body’s inflammatory load, but may also be acting directly in the liver and pancreas to cut insulin sensitivity.
“It is very hard to prove causation in a complex disease,” says Genco. We know that mice given a mouthful of P. gingivalis get gum disease – and diabetes, rheumatoid arthritis, atherosclerosis, fatty liver disease and Alzheimer’s-like symptoms. We know that, in humans, gum disease makes the other diseases more likely, and that P. gingivalis lurks in the affected tissues and makes the precise cellular changes typical of these conditions.
If these diseases actually share a more direct cause, it might finally suggest cures (see “Master of concealment“) – as well as explaining just how the same bad habits bring them all on. People who drink more alcohol tend to have more P. gingivalis and are more susceptible to gum disease. Tobacco smoke helps the bacteria to invade gum cells. Exercise, the only known way to lower your risk of Alzheimer’s, improves gum disease by damping inflammation and ending P. gingivalis’s feast.
Then there is diet. Douglas Kell at the University of Manchester, U.K., believes our blood contains many dormant bacteria, needing only a dose of free iron to awaken and cause disease. That could be why eating too much red meat and sugar or too little fruit and veg lead to these diseases: all increase your blood iron.
The long haul
No official medical advice for warding off these diseases includes “see your dentist”, at least not yet. “Periodontal disease should be better recognised by the community as a clearly established risk factor,” says Dominy. One of the clearest risks is for Alzheimer’s. But guidelines for avoiding Alzheimer’s published in May by the World Health Organization (WHO) say nothing about preventing gum disease.
“There is insufficient evidence to suggest that treating gum disease reduces the risk of dementia,” says Benoit Varenne at the WHO, echoing the verdict on heart disease, even though the same caveats probably apply. The guidelines recommend avoiding diabetes and high blood pressure, despite stating that there is little or no evidence that this stops Alzheimer’s.
“It’s perhaps too easy to mock the notion that flossing your teeth may contribute to good brain health,” says Margaret Gatz at the University of Southern California. And that may be part of why this idea hasn’t yet taken off in mainstream medicine. “There is a history of dental and medical doctors working apart and not cooperating,” says Thomas Kocher at the University of Greifswald, Germany.
But it also reflects the long-held belief that heart attacks and the other conditions are primarily the result of bad lifestyle, not bacteria. Such underlying paradigms in science can take decades to change. That happened when bacteria, not stress and stomach acid, were shown to cause stomach ulcers. After decades pursuing these explanations, many medical experts are reluctant to admit that amyloid may not cause Alzheimer’s and high cholesterol may not lead to heart disease.
With the world’s population ageing, we don’t have decades before these diseases become a health crisis severe enough to break health systems and societies. We need a new paradigm. That means facing the possibility that it may all be down to germs, after all.
Germ theory
A range of bacteria may play a role in supposedly non-communicable diseases. Propionibacterium acnes, for instance, is best known for causing acne, but also seems to damage the discs that cushion your spinal vertebrae, a common cause of severe back pain, says Ondrej Slab of Masaryk University in the Czech Republic. It has also been implicated in prostate cancer. But it is Porphyromonas gingivalis that has been linked to the widest array of conditions:
Rheumatoid arthritis
P. gingivalis is present in the joints of people who get this condition before symptoms appear and is the only bacterium known to make a chemical involved in the disease.
Parkinson’s disease
P. gingivalis and its protein-munching enzymes, gingipains, are found in the blood of people with Parkinson’s disease, and promote the inflammation and abnormal clotting seen in the condition.
Kidney disease
Gum disease is associated with chronic kidney disease and gum treatment seems to help the kidneys.
Fatty liver disease
There is far more P. gingivalis in affected livers than in healthy ones, and it worsens the disease in mice. Treating the gums helps.
Cancer
The bacteria has been found in early-stage cancers of the mouth, oesophagus, stomach and pancreas, and changes cell functions in ways typical of these cancers.
Macular degeneration
Injecting the bacteria into the retina seems to damage eyesight by producing age-related macular degeneration in mouse studies.
Gum disease, caused by P. gingivalis, has been established as a risk for premature birth.
It is here you may want to stop and catch your breath before you run off to brush your teeth. Cleaning your teeth is helpful but you may want to do a search on what’s called “Oil Pulling”. Oil pulling is using various oils to clean your teeth and gums deeply and without a brush. This requires time and patience. You put a tablespon or three of of oil into your mouth and DO NOT SWALLOW! Instead you swish it around in your mouth for 5 to 20 minutes. Sounds impossible…right?!? Wrong! It I.S. possible and incredibly effective! Once you see what you spit out when you’re done will quickly educate you in WHY you shouldn’t swallow! What goes in as nice, clean looking oil comes out as a disgusting, ugly, really gross looking oily gak similar to stuff you might see at the edge of an oil slick. You can rinse and/or brush afterward to remove the taste and residue. Your WHOLE mouth will never feel so clean!
particles or ions, which is best?
Antibacterial Activity and Mechanism of Action of the Silver Ion in Staphylococcus aureus and Escherichia coli.
The antibacterial effect and mechanism of action of a silver ion solution that was electrically generated were investigated for Staphylococcus aureus and Escherichia coli by analyzing the growth, morphology, and ultrastructure of the bacterial cells following treatment with the silver ion solution. Bacteria were exposed to the silver ion solution for various lengths of time, and the antibacterial effect of the solution was tested using the conventional plate count method and flow cytometric (F.C.) analysis. Reductions of more than 5 log10 CFU/ml of both S. aureus and E. coli bacteria were confirmed after 90 min of treatment with the silver ion solution. Significant reduction of S. aureus and E. coli cells was also observed by F.C. analysis; however, the reduction rate determined by F.C. analysis was less than that determined by the conventional plate count method. These differences may be attributed to the presence of bacteria in an active but nonculturable (A.B.N.C.) state after treatment with the silver ion solution. Transmission electron microscopy showed considerable changes in the bacterial cell membranes upon silver ion treatment, which might be the cause or consequence of cell death. In conclusion, the results of the present study suggest that silver ions may cause S. aureus and E. coli bacteria to reach an A.B.N.C. state and eventually die.
Since ancient times, the silver ion has been known to be effective against a broad range of microorganisms. Today, silver ions are used to control bacterial growth in a variety of medical applications, including dental work, catheters, and the healing of burn wounds. Silver ions are also used for a number of nonmedical purposes, such as in electrical appliances. The slow-release “nanosilver” linings of laundry machines, dishwashers, refrigerators, and toilet seats are also marketed and advertised. It is clear that we are exposed to a wide range of mostly unfamiliar uses of silver-containing products intended to function as antimicrobial biocides. Therefore, it is necessary to elucidate the antimicrobial activity of the silver ion, which is widely used in these products.
The mechanism of the antimicrobial action of silver ions is closely related to their interaction with thiol (sulfhydryl) groups ), although other target sites remain a possibility. Amino acids, such as cysteine, and other compounds containing thiol groups, such as sodium thioglycolate, neutralized the activity of silver against bacteria. By contrast, disulfide bond-containing amino acids, non-sulfur-containing amino acids, and sulfur-containing compounds, such as cystathione, cysteic acid, l-methionine, taurine, sodium bisulfate, and sodium thiosulfate, were all unable to neutralize the activity of silver ions. These and other findings imply that the interaction of silver ions with thiol groups in enzymes and proteins plays an essential role in its antimicrobial action, although other cellular components, like hydrogen bonding, may also be involved. Silver was also proposed to act by binding to key functional groups of enzymes. Silver ions cause the release of K+ ions from bacteria; thus, the bacterial plasma or cytoplasmic membrane, which is associated with many important enzymes, is an important target site for silver ions.
In addition to their effects on bacterial enzymes, silver ions caused marked inhibition of bacterial growth and were deposited in the vacuole and cell wall as granules. They inhibited cell division and damaged the cell envelope and contents of bacteria. Bacterial cells increased in size, and the cytoplasmic membrane, cytoplasmic contents, and outer cell layers all exhibited structural abnormalities. Finally, silver ions interact with nucleic acids (35); they interact preferentially with the bases in D.N.A. rather than with the phosphate groups, although the significance of this in terms of their lethal action is unclear.
The following silver compounds and silver are listed in Martindale: the Extra Pharmacopoeia: silver metal, silver acetate, silver nitrate, silver protein, and silver sulfadiazine. The silver ion can be generated by electrolyzing the silver metal or dissolving the silver compounds. It is known that the electrically generated silver ion appeared to be superior to the silver compounds in antimicrobial activity. However, most of the aforementioned studies which determined a mechanism of action of silver used silver ions produced from silver compounds like silver nitrate or silver sulfadiazine, and thus there has been limited research on the electrically generated silver ion. Recently, a laundry machine that emits electrically generated silver ions was developed for hygiene, namely, in order to prevent easily transmissible bacterial and fungal skin infections from being transmitted by contaminated laundry. In particular, it can be beneficial to hospitals and homes in which immunocompromised people (the elderly, children, and medical patients) or pets may dwell. Our previous study demonstrated the antifungal activity of a laundry machine that electrically generates silver ions. In the present study, we used conventional plate counting, flow cytometry (F.C.), and transmission electron microscopy (T.E.M.) to investigate the antibacterial activity and mechanism of action against Staphylococcus aureus and Escherichia coli bacteria of a silver ion solution generated from the laundry machine.It is known that the electrically generated silver ion appeared to be superior to the silver compounds in antimicrobial activity.
T.A.E.Z.Z.A.R. said:
I am still getting educated on colloidal silver.
I am a K.I.S.S. type person & therefore like the way Malus makes his.
Also:
I drink red wine from a 925 silver goblet.
Does the acidity of the wine take any silver from the goblet?
If so, how much ?
Hey guys, I am not being a wise ass, my question was sincere & legitimate.
I do not know & I an curious if the acidity in wine will leach out any silver
and if so is it the same as colloidal silver (have the same or similar benefits)?
I did find this bit of info:
Since the surface of silver is silver oxide (unless it’s been recently treated), you have a reaction between the acids in the wine with the silver oxide to form silver tartrate or silver malate/lactate. Those same salts, in turn, can react with any aldehydes or sugars present in the wine to form silver(0) again (the Tollens test) which will fall out of solution as a disperse black powder and promote oxidation to acetic acid and sugar lactones. None of this presents any human health hazard that I’m aware of, but could change the taste of the wine and detract from the appearance.
Goldbrix replied:
I think you are RESEARCHING just like we do. AND those of us here do not have an answer.
I do recall the sayings “Born with a silver spoon in his mouth.” and “Bluebloods”. Both indications of silver use in eating utensils. The former being a term for being Lucky, Rich or both.
I believe this saying was an observation from the common people, in this case during was the plague. The commoners noticed the upper class seemed less affected than they were. Commoners used wooden utensils and cups. Wood is a bacteria holder. The rich used silverware and goblets in comparison. It was also a common practice for God Parents to present a silver spoon to their God Child as a wish for prosperity and good health.
Just maybe the silver use was advantageous.
“Bluebloods” – Quality Control in earlier days was a problem and being so some silverware and cups produced were inferior. Those who had inferior silverware and drinking goblets may have had contamination and leaching issues. Those issues over time could have lead to slight cases or Argyria (blue skin) – hence “Blue Bloods”.
Wine and silver. – You may be onto something.
I keep an old, scratched up, oxidized silver coin in the dishwasher. The coin eventually appears clean and gets exchanged for another. No smells in the dishwasher itself. Whether it helps or not I do not know.
When I first got on a CPAP machine I noticed a floral smell (bacterial odor) build up after about a month of continual use. I started using CS/EIS in my CPAP water reservoir. The odor disappear almost over night probably 2nd or 3rd night I notice it was totally gone. I kept using CS/EIS in the reservoir until the metal heat element began to get a light black coating. I have stopped using the CS/EIS and just use distilled water. It has been over a year and a half and I have not had to clean any of the equipment, and I have not had to change tubing, or mask.
I keep a bottle of CS/EIS in a spray bottle for cleaning off the Kitchen Table and work surfaces the food lays on.
Anecdotal ? YES, But it works for me.
We Are ALL Researchers in this A.R.T. of CS/EIS.
Best of Luck,
Keep US Posted.
Thanks GOLDBRIX, even thou not too scientific, your info is interesting.
And yes, I am curious about a lot of stuff, so much that I don’t have enough
available time to properly research it all.Lost in Orygun.
I reply:
Goldbrix’s mention of the great plague and the possible role of silver in it encouraged me to read “Justinian’s flea.” It is a book that I heartily recommend. It examines the recurrence of plagues throughout history. Plagues are a phenomenon that repeats itself. After reading this book, the intelligent person will have a hard look at making their colloidal silver. Apart from the naturally occurring threats, consider the fact that there are thousands of crazy people willing to blow themselves up. It’s only a matter of time until some of these people acquire the expertise in microbiology to kill us more efficiently. Weaponizing microbes up to now has been limited by the time it takes the user to develop and deploy a vaccine so that he would not feel the effect of his device. That will not hinder the crazy people.
In Justinian’s Flea, William Rosen tells the story of history’s first pandemic—a plague seven centuries before the Black Death that killed tens of millions, devastated the empires of Persia and Rome, left a path of victims from Ireland to Iraq, and opened the way for the armies of Islam. Weaving together evolutionary microbiology, economics, military strategy, ecology, and ancient and modern medicine, Rosen offers a sweeping narrative of one of the great hinge moments in history.
I believe one of .GOVs alphabet agencies ordered those Silver Ion Generating Washing Machines off the US Market.
BUT
Since I make my own (Thanks Al) I drop a tablespoon of E.I.S. in the wash and in the liquid fabric softener. If one of the family members get sick with Cold or Flu symptoms I’ll kick it up to an ounce in both when I wash the sleep wear and bed linen.
and I run a cool mist vaporizer full of distilled water and one ounce of E.I.S. (15ppm +) in their bed room especially while they are in there sleeping. There does seem a quicker recovery and a lot fewer Dr. visits during the season. No Dr. Visits this past Cold and Flu Season. ( Must Be Something to it)
Aug 5, 2015#76
Hundreds sickened by contaminated cilantro from Mexico
Anything that you buy fresh to be eaten raw should be sprayed with or preferably soaked in colloidal silver.
A Belated Look at New York’s Cooling Towers, Prime Suspect in Legionnaires’ Outbreak
A bacteria, legionella, cause this. I don’t know whether or not colloidal silver would kill this particular bacteria. If it proved to be effective, it would be straightforward to install a colloidal silver generator powered by a solar panel on every water tower.
Feb 5, 2016#125
To treat a pending issue (cold, flu, etc…) The recommended serving I found is 1 tsp per day up to 10 days….. I spray it in my throat, use it for pink eye, skin wounds, yeast and fungal issues, tooth issues, any oral issues…. such a great cure-all, the general public is in the dark on this. Lots of info online- for other Survival Health (Holistic stuff) visit www.herbsholistics.com Right now, the shop has the most eye opening info. I discovered Usnea on this site, and now its a tincture we sell…. Interesting stuff, that herbal medicine! Colloidal Silver is a fantasic multipurpose antimicrobial which everyone should have in their Survival Health Arsenal!
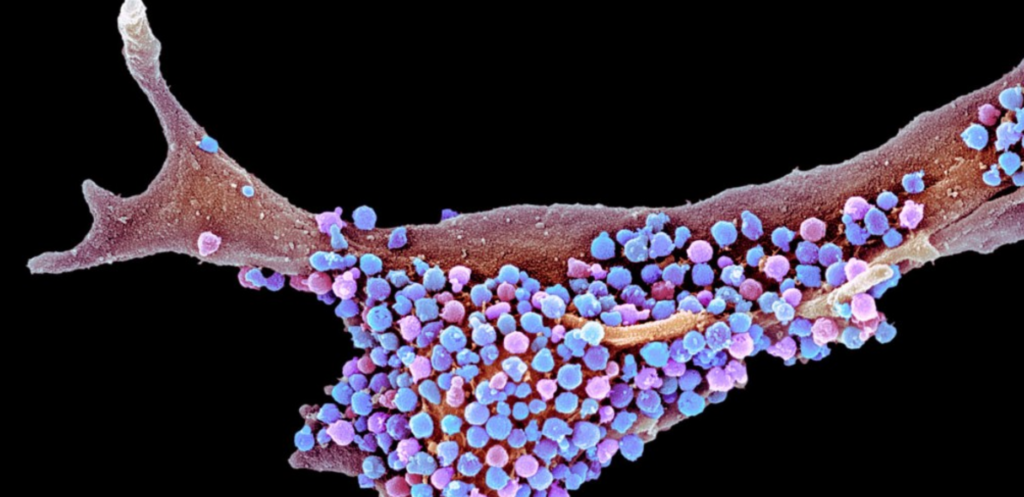
Some scientists think that microbes such as the herpes simplex virus 1 (shown here on an epithelial cell) could trigger some cases of Alzheimer’s disease. Credit: S.P.L.
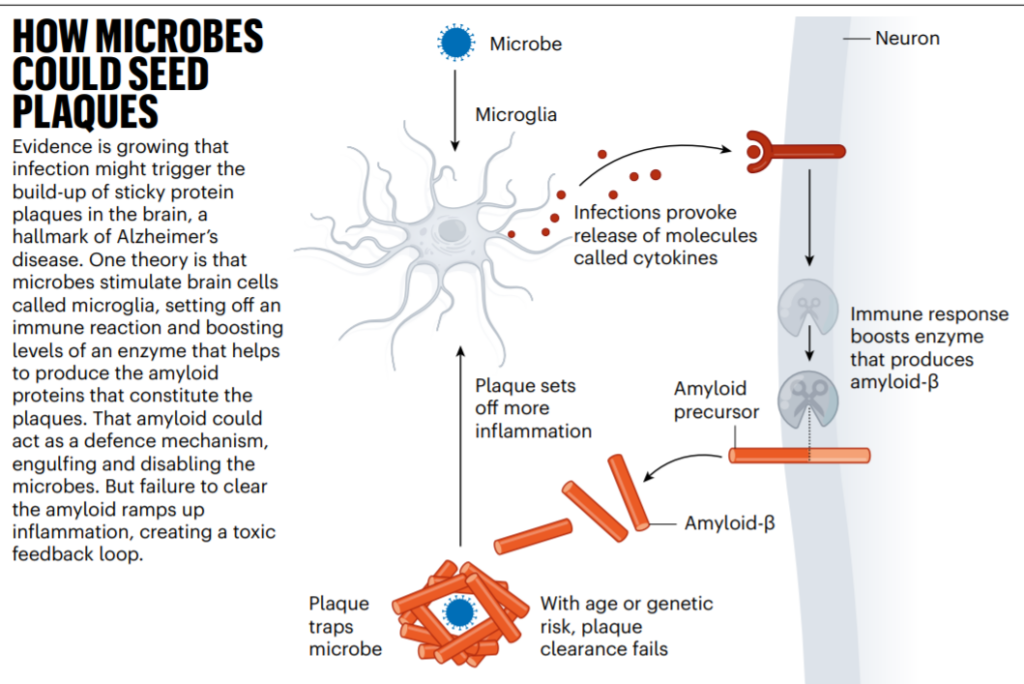
It would appear that plaques are a part of our immune system. Our immune system operates at the cellular level. It evolved without the knowledge that we would grow old. These deposits that serve to trap microbes before they can do us harm can, with age, interfere with our circulatory system and our nervous system. The brain is just another part of our nervous system. In my 30 years of experience with colloidal silver, I have been struck by the general good health and the mental acuity of the old-timers using colloidal silver, now E.I.S. Have a read of the entire article. It is not overly technical and shows that not everyone in medical research is a robot.
https://www.nature.com/articles/d41…ail&utm_term=0_c9dfd39373-fc6bf4b9de-43488673
Zarathushtra: “With an open mind, seek and listen to all the highest ideals. Consider the most enlightened thoughts. Then choose your path, person by person, each for oneself.”
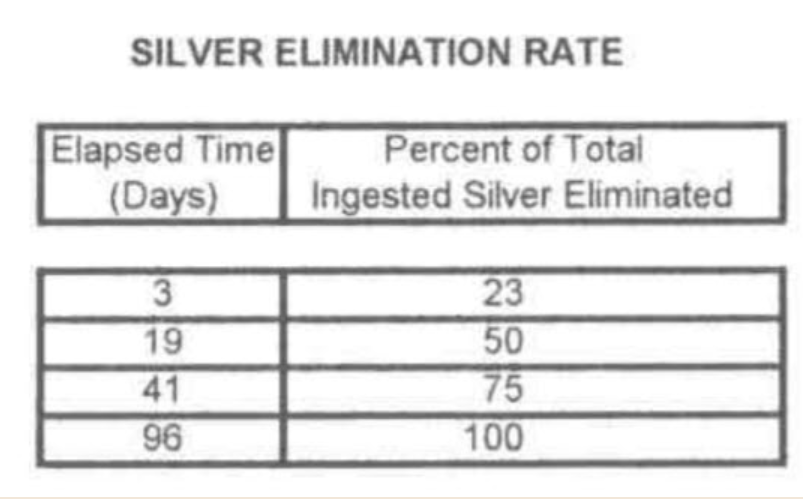
If your objective is to keep a certain amount of E.I.S. in your bloodstream as a front-line defense against pathogens (a brilliant move) then the following study is beneficial:
“What’s your opinion on small bottles of concentrated colloidal silver that come in brown bottles with an included eyedropper that one would use to put in distilled water?”
If someone tells you their colloidal silver is “concentrated,” you should stay away from them. It’s a sign that they are clueless. E.I.S., a.k.a. (colloidal silver) cannot be “concentrated.” It is not orange juice. If you’re talking about the stuff that sold in health food stores, forget about it, you have no idea what you’re going to get. If your wishes to see if colloidal silver will work for you, for instance for a sinus problem, you could try:
https://www.atlasnova.com/product/atlasnova-enhanced-colloidal-silver-50-ppm-4-oz/
If it works for you, you will know that you will be able to produce the same product if you purchase an ultra.
“Not sure if your smaller unit is big enough or the gallon or half gallon is too much, need your input, please.”
“Common” colloidal silver generators produce, at best, 10 to 15 ppm E.I.S. The ultras will do this in one day running in the 50 P.P.M. mode. It will be 98% ionic, completely clear and have a practically infinite shelf life. If you want 50 ppm, you will have to let it run for the full ten days. You can stop the process at any time. The LCD on the unit will tell you what the level of ionic P.P.M. is at all times during the process. You can stop the process at any point during the ten days, and you will have, 20, 30, 40 or whatever it is at that time. I would hope that my customers would get in the habit of starting a batch every ten days I’m just let it run until it’s finished. Then decant it into a storage container (glass) and put it away. Continue to do this until you have an excellent supply in case of an emergency. A burn, or plague, a sore that won’t heal, a strange rash, sinus infection, pinkeye or whatever you think it might help. At least, it won’t do any harm. As to which unit to buy, the one and a half pint or the half gallon, it depends on your situation. Are you alone? Then perhaps the one and a half pint would do. For a family, I would suggest a half gallon to be a better investment. It only cost 50% more, yet it produces almost three times the volume of 50 ppm.
Jul 14, 2020#847
Promising cure to URTI pandemics, including the Avian Flu (H5N1): has the final solution to the coming plagues been discovered?
Recently Rentz (2003) published a convincing retrospective, peer-reviewed treatise on a highly advanced, effective and safe virotoxic oligodynamic silver ([Ag.sup.+]) hydrosol, making the case that it is the agent of choice to combat SARS. (1) The works of Goetz (1940), (2) Berger et al (1976), (3) Simonetti et al (1992), (4) Russel et al (1994), (5) and Crocker and Grier (1998) (6) collectively established that electrolytically produced oligodynamic [Ag.sup.+] hydrosol provides the ideal speciation of bioactive [Ag.sup.+] completely harmless to mammals, in contrast to other colloidal silver or silver salt speciations that are predominantly inactive and potentially toxic to mammals. They also established that oligodynamic [Ag.sup.+] hydrosol possesses fabulous virotoxic properties. Comprehensive studies conducted by NASA (circa 1970) on a crude oligodynamic [Ag.sup.+] hydrosol preparation offer a compelling argument that today’s highly advanced oligodynamic [Ag.sup.+] hydrosols may be the solution to lessening the impact of viral plagues. With today’s advancement in [Ag.sup.+] processing technology, at least one commercially available, cost-effective oligodynamic [Ag.sup.+] hydrosol is (a) proven to be over 95% bioactive per volume, with (b) an unprecedented surface area of activity (i.e., 6 [km.sup.2] per gram Ag), that provides (c) an ideal concentration factor of < 25 ppm, in (d) an ideal liquid medium.
CONCLUSION: The pharmacology of advanced oligodynamic [Ag.sup.+] hydrosol shows great promise to easily overwhelm key defensive mechanisms of URTI resistance in general, including H5N1. Additional clinical studies are warranted to further demonstrate the efficacy and compatibility of per os virotoxic oligodynamic [Ag.sup.+] hydrosol, as well as investigational intravenous and nebulized (aerosol) protocols.
Key words: URTI pandemics, H5N1, oligodynamic [Ag.sup.+] hydrosol pharmacology, microbial defenses, microbial resistance, conventional treatments, effective protocol development, hyposmolarity, sorbitol.
Introduction
During the past 300 years, humanity has suffered ten pandemics and several epidemic scares. Could the solution to pandemics have a simple answer? Has nature always held the key to defeating pathogens in a simple [Ag.sup.+] molecule?
Commonly known as the flu or the grippe, influenza is a contagious disease of the upper respiratory tract caused by viruses from the orthomyxoviridae family, all R.N.A. viruses. (7) Generally, human Influenzavirus starts with direct human contact with sick poultry and other animals. (8,9)
The orthomyxoviridae family is divided into three types–Influenzavirus A, B, and C. Each type is differentiated by its respective “antigenic” nucleoprotein and matrix protein dissimilarities. (10)
Because two main “antigenic” surface glycoproteins of Influenzavirus A are prone to significant mutation, this virus requires further classification into subtypes. The Influenza A virus is a species of the genus influenzavirus A. There are multiple subtypes of Influenza A. The H5N1 virus is a direct descendent of the Spanish Flu virus, a subtype of Influenza A. Influenzavirus B and C do not have subtypes. However, Influenzavirus B and the subtypes of Influenzavirus A are further classified into strains. (11) The H5N1 subtype alone has more than 400 different strains. (12) Only Influenzavirus A may cause pandemics.
Viruses cause most upper respiratory tract infections (URTIs), such as adenovirus, coronavirus, coxsackievirus, influenza virus, parainfluenza virus, respiratory syncytial virus, and rhinovirus, which account for the majority of cases. (1) A broad-spectrum anti-viral agent that really works is needed to combat over 200 viruses that cause URTIs. (2) Undoubtedly oligodynamic silver fits this bill.
Emerging medical studies confirm the stellar, broad-spectrum virotoxic efficacy of oligodynamic silver both in vitro and in vivo. This includes some of the most formidable viral organisms like H.I.V. (including co-infections) (3-11) and Herpesvirus hominis (HSV). (12-18) Despite the low yields of oligodynamic silver of the past 100 years common to silver-based drugs, the collective authoritative medical literature has documented efficacy of silver’s virotoxicity against over 24 viruses. For the viruses relevant to URTIs, the following are known to succumb to oligodynamic silver:
Oligodynamic silver’s antimicrobial efficacy extends well beyond its virotoxicity. Oligodynamic silver’s lethal effects span across all microbial domains (viral, bacterial, and fungal). The following URTI-related bacteria are known to be susceptible to oligodynamic silver:
Case History
Perhaps oligodynamic silver’s most compelling nature lies in its ability to successfully eradicate pervasive primary and secondary co-infections simultaneously. A major, double-blind, controlled trial concerning advanced AIDS candidiasis and immunity-suppressing moieties demonstrated complete sero-negative conversion after a single treatment with oligodynamic silver hydrosol! The studies were conducted at Lucha Contra el Sida, Comayaguela, Tegucigalpa, Honduras, Central America.
Quoting from the study, “Furthermore, said devices [silver oxide hydrosol] are capable of killing pathogens and purging the bloodstream of immune suppressing moieties (I.S.M.) whether or not created by the AIDS virus (H.I.V.), so as to restore the immune system.” (86) (Brackets added by authors.)